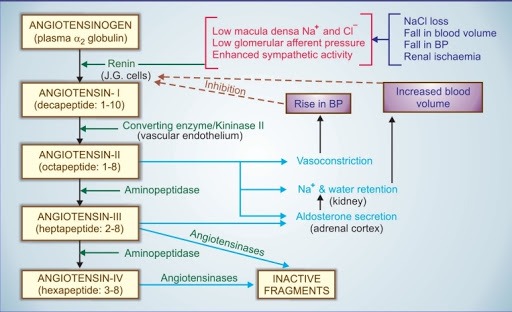
Circulating renin-angiotensin system
Tissue (local) renin-angiotensin systems :
Extrinsic local RAS: Blood vessels can also produce Angiotensin II apart from circulation
Intrinsic local RAS: Many tissues can also produce all components of the Renin-Angiotensin System, eg: Heart, Blood vessels, Brain, Kidneys, Adrenals. Here the system regulates cell growth, cell death, remodeling, fibrosis.
- Circulating RAS synthesize – RENIN
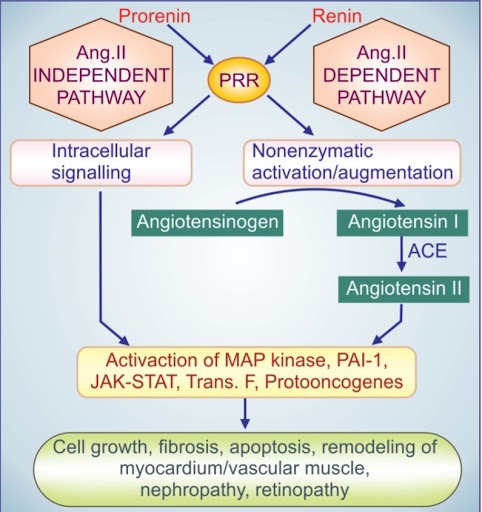
- Local RAS tissues synthesize -PRORENIN
(concentration of prorenin and renin in circulation = 5 to 10 : 1 ) Prorenin is activated by Enzymatically and Non-enzymatically.
Enzymatic activation – proteases like proconvertase-1 and Cathepsin B cut off the ‘propeptide’ to produce renin. This makes catalytic exposion of renin. This is a irreversible activation.
Nonenzymatic activation – occurs by binding of prorenin to (PRR) (Pro) renin receptor.This binding brings about a conformational change, the ‘propeptide’ segment detached and the catalytic domain is exposed. This activation is reversible. While renin binds to PRR, augmentation of catalytic activity of renin into several folds happens. In local RAS Nonenzymatic activation of prorenin plays a major role, the effects of prorenin exerted through 2 pathways
- AT1 – Losartanis a selective Antagonist
- AT2 – PS123177 is a selective Antagonist
- Intrarenal baroreceptor pathway: These decrease afferent glomerular arterioles tension and it operates via increased production of prostaglandins (PGs) and stretches sensitive ion channels.
- Macula densa pathway: Macula densa cells triggers this pathway. It has been found that COX-2 and neuronal nitric oxide synthase (nNOS) are induced in macula densa cells. These induce the release of PGE2 and PGI2. The locally released PGs act on juxtaglomerular cells to promote renin secretion.
- Beta adrenoceptor pathway: Baroreceptor and other reflexes that increase sympathetic impulses to JG cells activate Beta1 adrenoceptors expressed on their surface –> increased intra- cellular cAMP triggers renin release.
- Long loop negative feedback mechanism
- Short loop negative feedback mechanism
Renin release enhancers
- ACE inhibitors,
- AT1 Antagonist,
- Vasodilators,
- Diuretics,
- Loop diuretics
Renin release inhibitors
- Central Sympatholytics
- Beta blockers
- NSAIDs
- COX – 2
- Sympathetic blockers – Beta-blockers, adrenergic neuron blockers, central Sympatholytics
- Direct renin inhibitors – e.g. aliskiren
- Angiotensin converting enzyme inhibitors – e.g. captopril
- Angiotensin receptor blockers – e.g. losartan
- Aldosterone Antagonist – e.g. spironolactone
I’m Nawin (Admin), a seasoned doctor and accomplished content writer with 8 years of experience. Join me as I unravel the latest breaking news, unveil behind-the-scenes happenings, and explore the aftermath scenes. With my expertise, I’ve crafted this renowned news site to provide you with an authentic perspective on daily happenings. Get ready to delve into a world of truth and knowledge on Medico Topics.